

Ijraset Journal For Research in Applied Science and Engineering Technology
A Retrospective Analysis on Clinical Characterization and Post-Operative Complication of Patient with Inguinal Hernia in Single Centred Health Care Setting
Authors: P. Nithiya Kala, Merlin Jose, B. Monica , M. Gayathri, R. Muthu Selvi
DOI Link: https://doi.org/10.22214/ijraset.2022.47082
Certificate: View Certificate
Abstract
Background An inguinal hernia is a common condition associated with advanced age, male gender, risk factors and clinical characteristics.A hernia occurs when an organ pushes through an opening in the muscle or tissue that holds it in place. It protrudes through bodily parts due to abnormalities in the anatomical structures that ordinarily contain it. Objectivethis study is aimed to clinical characterization and post-operative complication of patient with inguinal hernia. Methodology: The study was a single-centred retrospective cross-sectional study. The study was performed on patients with inguinal hernia and those who underwent inguinal hernia repair at Vivekanandha Medical Care Hospital in Tiruchengode from March 2022 to May 2022. A total of 62 patients were enrolled in the study based on inclusion and exclusion criteria the data is collected through chart review of existing medical record of study site. Results: The participants were primarily in the 40–59 age range (41%), and gender indicated significant disparities, with more male patients than female patients. Inguinal hernias more frequently affect active employees than sedentary ones. The majority of them were overweight (42%) with normal weight (40.3%), obesity (12.9%), and underweight (4.8%) following closely behind. The most prevalent risk factors were persistent constipation. Conclusion:A complete physical examination and history are used to diagnose the majority of inguinal hernias
Introduction
I. INTRODUCTION
A hernia occurs when an organ pushes through an opening in the muscle or tissue that holds it in place. It protrudes through bodily parts due to abnormalities in the anatomical structures that ordinarily contain it. The abdomen is the most commonly affected area. Abdominal wall hernia are more prevalent, accounting for around 15-18% of all operative methods1, 2.
Effectively, any risk factor that raises intra-abdominal pressure or weakens the front abdominal wall may result in the establishment of an inguinal hernia3.For example, chronic cough, chronic obstructive pulmonary disease, chronic constipation, benign prostatic hyperplasia, family history of hernia, collagen diseases, previous right lower quadrant incision, smoking, physical activity, and bearing the burden may be named.4,5
Inguinal hernia repair is one of the most common procedures performed worldwide, with over 20 million patients undergoing the procedure each year
The lifetime prevalence of groin hernias (visceral or adipose tissue protrusions through the inguinal or femoral canal) in males is 27-43 percent and 3-6 percent in women.6, 7Inguinal hernias are almost always symptomatic, and the only cure is surgery. Therefore it is successful in the majority of cases. 6
There are two primary surgical methods: open surgery and laparoscopic. There are several ways for repairing the herniation site, the most common of which are classical and preperitoneal.
The classical approach is the gold standard in herniorrhaphy and is simpler than alternative methods of treatment used by most surgeons (8-10). In this method, the mesh is placed on the base of the inguinal canal, under which is inserted the thin transverse abdominal fascia. As a result, it creates a relapse-prone region.
The preperitoneal approach, on the other hand, reduces recurrence rates since the mesh is implanted beneath the fascia and on the peritoneum (11, 12)
II. METHODOLOGY
The study was a single-centred retrospective cross-sectional study. The study was performed on patients with inguinal hernia and those who underwent inguinal hernia repair at Vivekanandha Medical Care Hospital in Tiruchengode from March 2022 to May 2022. A total of 62 patients were enrolled in the study based on inclusion and exclusion criteria. Patients aged 20 and above, individuals who underwent inguinal hernia repair, patients with primary or recurrent hernia, and patients with post-operative complications were included in the study. Patients of less than 20 years of age, cardiac patients or immunosuppressive patients were excluded from the study.
The information and data were gathered through a chart review of the study site's existing medical records. Detailed demographic details such as age, gender, occupation, BMI, risk factors/past medication history etc. were collected along with the clinical presentation of hernia and also post-operative complications. All the relevant data was filled into Microsoft Excel, and the analysis was done with the graphs and tables.
III. RESULT
A sum of 62 patients was enlisted in the study based on both inclusion and exclusion criteria.
Table 1: Socio-Demographic data distribution
|
Socio-Demographic Data |
Variables |
Frequency |
Percentage |
|
Age |
20-39 Years |
14 |
22% |
|
40-59 Years |
29 |
47% |
|
|
Above 60 Years |
19 |
31% |
|
|
Gender |
Male |
58 |
94% |
|
Female |
4 |
6% |
|
|
Occupation |
Strenuous workers |
40 |
65% |
|
Sedentary workers |
22 |
35% |
|
|
BMI |
Underweight |
3 |
4.8% |
|
Normal |
25 |
40.3% |
|
|
Overweight |
26 |
42% |
|
|
Obese |
8 |
12.9% |
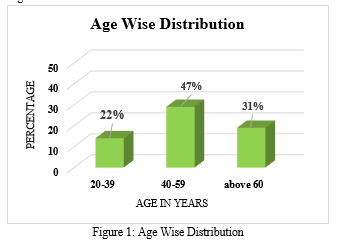
A. Age Wise Distribution
Among 62 patients, the predominant age group were 40-59 (47%), than other age group, followed by age group above 60 (31%).And the least number of participants were age group 20-39 (22%).In our study participants predominantly with age group 40-59 was described in table 1 and figure 1.
 \
\
V. CATEGORISATION OF CLINICAL PRESENTATION OF INGUINAL HERNIA
Among the participants, majority were presented with right inguinal hernia 24(38.7%) followed by left inguinal hernia 22(35.5%) and bilateral hernia 16(25.8%) and majority of participants were having reducible hernia 32(35.5%) followed by irreducible hernia 18(29.0%),incarcerated hernia 8(13%) and least number of participants had strangulated hernia 4(6.4%). 44 (71%) of patients had primary hernia while 18(29%) were having recurrent hernia was described in table 3.
Table 3: Clinical presentation of inguinal hernia
|
Clinical Presentation data
|
Variables |
Frequency |
Percentage |
|
Position of Hernia |
Left |
22 |
35.5% |
|
Right |
24 |
38.7% |
|
|
Bilateral |
16 |
25.8% |
|
|
Type of Hernia |
Reducible |
32 |
35.5% |
|
Incarcerated |
8 |
13% |
|
|
Irreducible |
18 |
29.0% |
|
|
Strangulated |
4 |
6.4% |
|
|
Classification based on recurrence |
Primary Hernia |
44 |
71% |
|
Recurrent Hernia |
18 |
29% |
VI. POST OPERATIVE COMPLICATION OF INGUINAL HERNIA
Among 62 participants, majority of patients did not develop any postoperative complication whereas 16(25.8%) patients developed post-operative complication, hematoma 6(9.7%) and wound infection 6(9.7%) was the main post-operative complication, least number of participants developed with wound site pain 2(3.2%), scrotal swelling 1 (1.6%) and Orchitis 1(1.6%) was described in table 4 and figure 6.
Table 4: Post-operative complication of inguinal hernia repair
|
Post-operative complication of Hernioplasty |
Variables |
Frequency |
Percentage |
|
Hematoma |
6 |
9.7% |
|
|
Wound Infection |
6 |
9.7% |
|
|
Wound site pain |
2 |
3.2% |
|
|
Scrotal Swelling |
1 |
1.6% |
|
|
Orchitis |
1 |
1.6% |
|
|
Nil |
46 |
74.2% |
VII. DISSCUSSION
Inguinal hernias are prevalent surgical issue, although they can be devastating. The prevalence of inguinal hernia increase with age. In our study, majority of patients belongs to age group 40-59 years were the most commonly affected. This result was similar to the study conducted byBalamaddaiah G et al13.,the study revealed that, the most common affected age group was 46-60 years followed by 30-45 years.
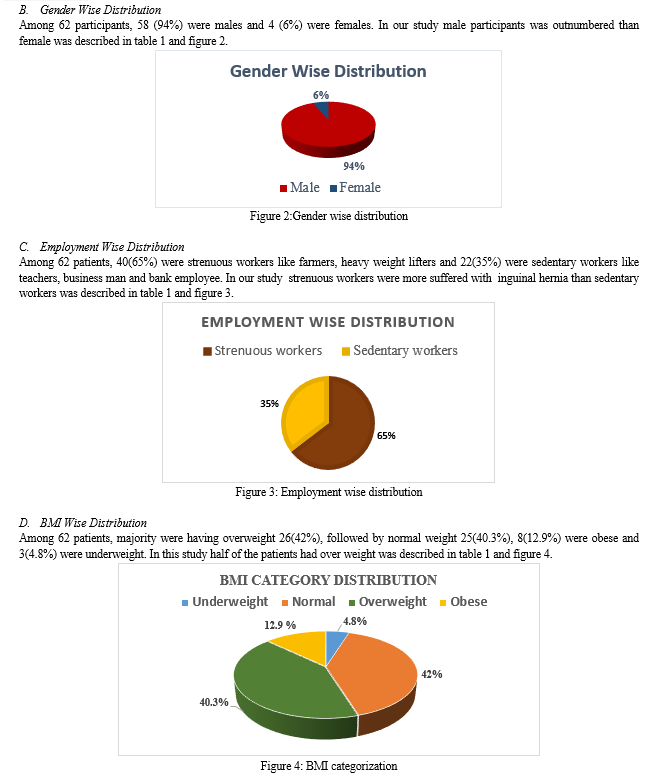
A total of 62 patients were included in this study.Inguinal hernia affects men more frequently than women. Among them (94%) were males and (4%) were females. Gender showed significant differences, with males patients were outnumbered than the females. This result was similar to the study conducted by A. Z. Khalaf et al14 .,the study revealed that majority of patients were male, which may be due to the abdominal wall's intrinsic weakness where the spermatic cord crosses through the inguinal canal.
The study reveals that strenuous worker are most commonly affected by inguinal hernia than sedentary workers the study was similar to the study conducted byBalamaddaiah G et al13showed the most common cause for the presence of hernia was lifting heavy objects i.e. strenuous workers are more likely to have hernia than sedentary workers.
The present study depicted to the BMI distribution of the patients revealed that majority of them were havingoverweight (42%) followed by normal weight (40.3%), obese (12.9%) and underweight (4.8%).The study was unlike to the study conducted by Sundar et.al.,15 the study revealed that majority of population belongs to BMI group 18.5-22.9 kg/m2 and lowest in ≥30 kg/m2 .The prevalence of inguinal decreased as the BMI category increased and vice versa
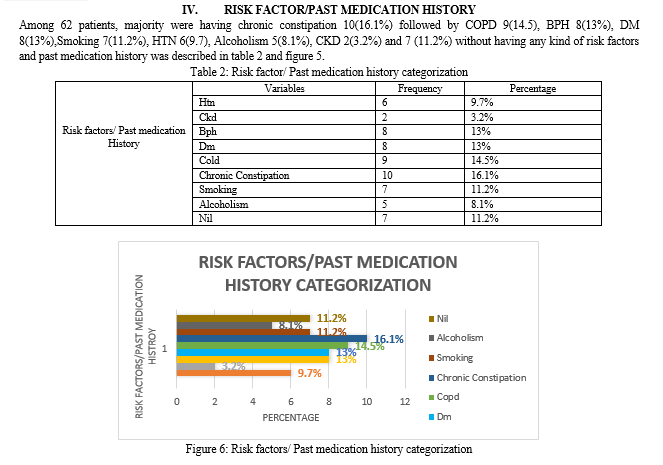
The study observed that chronic constipation was most common risk factors (16.1%), followed byCOPD 9(14.5), BPH 8(13%), DM 8(13%),Smoking 7(11.2%), HTN 6(9.7), Alcoholism 5(8.1%), CKD 2(3.2%) and 7 (11.2%) without having any kind of risk factors and past medication history, The study was dissimilar to the study conducted bySundar et al.,15 the study revealed that most Common risk factors responsible for the inguinal hernia were: smoking ,chronic cough ,heavy work and COPD
While assessing the clinical presentation of inguinal hernia, Among the participants, majority were presented with right inguinal hernia 24(38.7%) followed by left inguinal hernia 22(35.5%) and bilateral hernia 16(25.8%), the study was similar to the study conducted by Gulzar MR et.al.,16 the study revealed that majority patient had right-sided hernia, fewer had left-side hernia, while bilateral hernia was the least common. Majority of participants were having reducible hernia 32(35.5%) followed by irreducible hernia 18(29.0%), incarcerated hernia 8(13%) and least number of participants had strangulated hernia 4(6.4%). 44 (71%) of patients had primary hernia while 18(29%) were having recurrent hernia.
The study observed that majority of patients did not develop any postoperative complication whereas 16(25.8%) patients developed post-operative complication, hematoma 6(9.7%) and wound infection 6(9.7%) was the main post-operative complication, least number of participants developed with wound site pain 2(3.2%), scrotal swelling 1 (1.6%) and Orchitis 1(1.6%),the study was similar Chan Yong Park, et al.,17the study revealed that most commonpost-operative complication, was hematoma and wound infection.
Conclusion
A complete physical examination and history are used to diagnose the majority of inguinal hernias. The socio –demographic result obtained from this study shows that 41-59 years old male overweight and strenuous working patients are most predominantly affected by inguinal hernia. The most common clinical characteristics such as chronic constipation, right position, reducible and primary hernia. The majority of the patients have no post-operative complication of hernioplasty. The most important risk factors such as overweight and heavy weight lifting increases the strain and pressure on the abdominal muscles and make them weaker and prone to developing hernias.
References
[1] Mebula JB, Chalya PL. Surgical management of inguinal hernias at Bugando medical centre in northwestern Tanzania: our experience in a resource-limited setting. BMC Research Notes. 2012;5:585. [2] Primatesia P, Golacre MJ. Inguinal hernia repair, incidence of elective and emergency surgery. Int J Epidemiology. 1996;25:835-9. [3] Simons MP, Aufenacker T, Bay-Nielsen M, Bouillot JL, Campanelli G, Conze J, et al. European Hernia Society guidelines on the treatment of inguinal hernia in adult patients. Hernia. 2009; 13(4):343-403. [4] Abramson JH, Gofin J, Hopp C, Makler A, Epstein LM. The epidemiology of inguinal hernia. A survey in western Jerusalem. Journal of Epidemiology & Community Health. 1978 Mar 1;32(1):59-67. [5] D. Neuhauser, Elective Inguinal Herniorrhaphy Versus Truss in the Elderly, Oxford University Press, 1977. [6] HerniaSurge Group: International guidelines for groin hernia management. Hernia 2018;22:1-165. [7] Kingsnorth A, LeBlanc K: Hernias: inguinal and incisional. Lancet 2003;362:1561-1571. [8] Amid PK. Lichtenstein tension-free hernioplasty: its inception, evolution, and principles. Hernia. 2004 Feb;8(1):1-7. [9] Kurzer M, Belsham PA, Kark AE. The Lichtenstein repair for groin hernias. Surgical Clinics. 2003 Oct 1;83(5):1099-117. [10] Sakorafas GH, Halikias I, Nissotakis C, Kotsifopoulos N, Stavrou A, Antonopoulos C, Kassaras GA. Open tension free repair of inguinal hernias; the Lichtenstein technique. BMC surgery. 2001 Dec;1(1):1-3. [11] Lichtenstein IL, Shulman AG, Amid PK, Montllor MM. The tension-free hernioplasty. The American Journal of Surgery. 1989 Feb 1;157(2):188-93. [12] Muldoon RL, Marchant K, Johnson DD, Yoder GG, Read RC, Hauer-Jensen M. Lichtenstein vs anterior preperitoneal prosthetic mesh placement in open inguinal hernia repair: a prospective, randomized trial. Hernia. 2004 May;8(2):98-103. [13] Balamaddaiah G, Reddy SR. Prevalence and risk factors of inguinal hernia: a study in a semi-urban area in Rayalaseema, Andhra Pradesh, India. International Surgery Journal. 2016 Dec 9;3(3):1310-3. [14] Ahmed Ziarra Khalaf (2021) Pattern of inguinal hernia in Al- Basra teaching hospital: a prospective clinical study, Alexandria Journal of Medicine, 57:1, 70-74 [15] Shrestha S, Upadhyay PK. Prevalence of Obesity in Inguinal Hernia Repair Patients in a Tertiary Care Center. JNMA: Journal of the Nepal Medical Association. 2021 Feb;59(234):156. [16] Gulzar, MR, Iqbal J, Ulhaq MI, Afzal M. Darning vsbassini repair for inguinal hernia: a prospective comparative study. Professional Med J. 2007;14:128-33. [17] Park CY, Kim JC, Kim DY, Kim SK. Inguinal hernia repair in overweight and obese patients. Journal of the Korean Surgical Society. 2011 Sep 1;81(3):205-10.
Copyright
Copyright © 2022 P. Nithiya Kala, Merlin Jose, B. Monica , M. Gayathri, R. Muthu Selvi. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.

Download Paper
Paper Id : IJRASET47082
Publish Date : 2022-10-15
ISSN : 2321-9653
Publisher Name : IJRASET
DOI Link : Click Here
 Submit Paper Online
Submit Paper Online