

Ijraset Journal For Research in Applied Science and Engineering Technology
A Review on Fungal Disease: Mucormycosis
Authors: Dhiraj Mundhe, Dr. Rupali Tasgaonkar, Prof. Gayatri Sapkale, Sanskruti Lokhande, Kasturi Turde, Manali Dhule
DOI Link: https://doi.org/10.22214/ijraset.2023.48986
Certificate: View Certificate
Abstract
As the fight against the deadly Covid 19 pandemic continues worldwide, several complications were being reported in patients who have recovered from Covid. One such deadly complication that has been reported recently in patients in India who were tested positive for Covid-19 and are gradually recovering was a fungal disease called mucormycosis, or black fungus. As hundreds of cases had been reported across the country, this had caused an additional wave of panic among the population. Post-Covid-19 patients who are more susceptible to mucormycosis are those with a history of poorly controlled diabetes mellitus and also those who are immunocompromised and have been treated with steroids and other medications for Covid-19. This brief review briefly discusses the epidemiology of mucormycosis, its potential pathophysiology in the post-Covid scenario, its clinical presentation, and its diagnosis and treatment. This brief review briefly discusses the epidemiology of mucormycosis
Introduction
I. INTRODUCTION
A. History
The primary cause of mucormycosis was probably one defined with the aid of Friedrich oküchenmeister in 1855. Fürbringer first defined the disease inside the lungs in 1876.[14] In 1884, Lichtheim set up the development of the sickness in rabbits and defined species; Mucor corymbifera and Mucor rhizopodiformis, later called Lichtheimia and Rhizopus, respectively.[15] In 1943, its association with poorly controlled diabetes became mentioned in three cases with severe sinus, brain, and eye involvement.[14]
In 1953, vasiform, found to motivate numerous cases, became isolated from Indian forest soil, and in 1979, P. C. Misra tested soil from an Indian mango orchard, from which they remoted Apophysomyces, later determined to be a first-rate motive of mucormycosis.[14] numerous species of Mucorales have for this reason that been described.
[14] whilst cases were mentioned inside the u.S.A. Within the mid-Nineteen Fifties, the author notion it to be a brand new disease on account of the use of antibiotics, ACTH, and steroids.[15][16] till the latter half of the twentieth century, the most effective to be had treatment was potassium iodide. In a review of cases regarding the lungs recognized following flexible bronchoscopy between 1970 and 2000, survival was discovered to be higher in those who obtained blended surgical operation and medical remedy, typically with amphotericin B.[15]
B. Mucormycosis
Mucormycosis (formerly known as zygomycosis) is a severe but uncommon fungal contamination because of a collection of molds referred to as micromycetes.
[1] Mucormycosis is an angioinvasive sickness because of saprophytic fungi of the order Mucorales. [4] The expected prevalence of mucormycosis is around 70 times better in India than that in international facts.[4] Diabetes mellitus is the maximum not unusual chance element, accompanied by using hematological malignancy and stable-organ transplant.[4] Mortality associated with invasive mucormycosis is excessive (> 30-50%), with 90% mortality related to the dispersed sickness.[5] Mortality rates are plenty decrease, even though still full-size (10-30%), amongst patients with localized cutaneous sickness.[5] Mucorales have a deviating histological look, with abnormal, non septate hyphae that department at right angles.[5] they may be greater, not unusual in soil than in air, and in summer season and fall than in winter or spring.[1,6] most of people come in contact with microscopic fungal spores every day, so it’s probably impossible to completely avoid coming in contact with micromycetes.[1,6] those fungi aren’t harmful to most of people.
However, for humans who've weakened immune structures, inhaling micromycetes spores can purpose contamination inside the lungs or sinuses which can spread to other parts of the frame.[1,10] several distinct varieties of fungi can cause mucormycosis.[1,10] those fungi are known as micromycetes and belong to the medical order Mucorales.[1] The most commonplace types that reason mucormycosis are Rhizopus species and Mucor species. Other examples encompass Rhizomucor species, Syncephalastrum species, Cunninghamella bertholletiae, Apophysomyces Lichtheimia (formerly Absidia), Saksenaea, and Rhizomucor.[1,10]
C. Types of Mucormycosis
- Rhino cerebral (sinus and brain) mucormycosis is contamination inside the sinuses that could unfold to the brain. This is not unusual in humans with uncontrolled diabetes and people with kidney transplants. [1,6]
- Gastrointestinal mucormycosis is more commonplace amongst younger kids than adults. Premature and low-delivery-weight babies much less than 1 month of age are at hazard in the event that they have had antibiotics, surgical procedures, or medicinal drugs that decrease the body’s ability to fight germs and sickness [1,7]
- Pulmonary (lung) mucormycosis is the most not unusual type of mucormycosis in human beings with most cancers and in humans who have had an organ transplant or a stem mobile transplant. [1,7]
- Cutaneous (skin) mucormycosis occurs after the fungi enter the frame via a smash within the pores and skin. This kind of infection might arise after a burn, scrape, cut, surgery, or different forms of pores and skin trauma. That is the most not unusual form of mucormycosis amongst those who do not have weakened immune systems. [1,6]
- Disseminated mucormycosis takes place while the infection spreads via the bloodstream to have an effect on every other part of the body. The contamination maximum generally affects the brain but can also have an effect on other organs together with the spleen, heart, pores, and skin. [1,6]
Symptoms of Mucormycosis
The signs of Mucormycosis depend on wherein the fungus is growing in the frame.[3] the two most critical types of Mucormycosis in this scenario are rhino-orbital-cerebral and pulmonary. [3] symptoms of rhino cerebral (sinus and brain) mucormycosis are One-sided facial swelling, Headache, Black lesions at the nasal bridge or top inner of the mouth that quickly turn out to be greater excessive, and fever. [1,7] signs and symptoms of pulmonary (lung) mucormycosis encompass fever, cough, chest ache, shortness of breath, Gastrointestinal bleeding, nausea vomiting. [1,8] Disseminated mucormycosis clearly takes place in those who are already ill from different medical situations, so it can be difficult to realize which signs are associated with mucormycosis. Patients with dispersed contamination inside the mind can increase intellectual reputation changes or coma.[1,8]
D. Culture and Biopsy
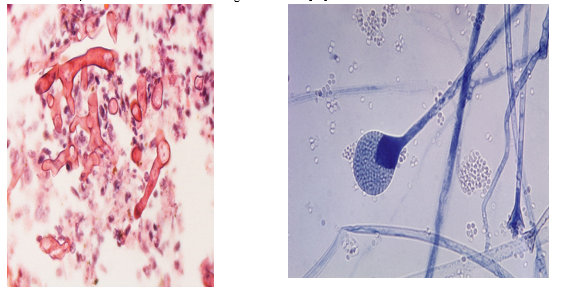
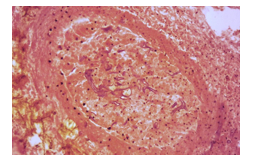
To verify the diagnosis, biopsy samples can be cultured.[10] tradition from biopsy samples does now not usually provide a result because the organism is very fragile. To exactly become aware of the species’ calls for a professional.[11] the appearance of the fungus under the microscope will decide the genus and species.[9] The appearances can range however commonly display wide, ribbon-like filaments that normally do now not have septa and that not like in aspergillosis—branch at proper angles, resemble antlers of a moose, which can be seen to be invading blood vessels.[11]
E. Mechanism
Mucormycosis is normally unfold through inhaling, ingesting meals infected by way of, or getting spores of molds of the Mucorales type in an open wound.[7] It isn't always transmitted among human beings.[8] the suitable mechanism by means of which diabetics end up inclined is unclear. In vivo, an excessive sugar degree alone does now not allow the boom of the fungus, however, acidosis by myself does. Human beings with excessive sugar degrees regularly have excessive iron ranges, also recognized to be a chance component for growing mucormycosis.[11] In people taking deferoxamine, the iron removed is captured via siderophores on Rhizopus species, which then use the iron to develop.[11]
II. MUCORMYCOSIS OCCURRENCE AND INCIDENCE IN INDIA
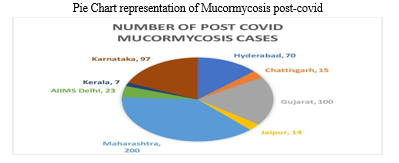
Overall, 526 cases of mucormycosis post-COVID-19 have been reported, of which 200 cases were from Maharashtra, 100 from Gujarat,97 from Karnataka,70 from Hyderabad, and 14,15,07,23 respectively from Jaipur, Chattisgarh, Kerala, and Delhi.[2] Mucormycosis was mainly seen in males (37%), (and 63%) in females. The data indicates that the estimated prevalence of mucormycosis in India is nearly 70 times higher than the global data, which were estimated to be at 0.02 to 9.5 cases (with a median of 0.2 cases) per 100,000 persons.[4]
III. CLINICAL MANIFESTATIONS AND DIAGNOSIS
The signs and symptoms of Mucormycosis rely on where the fungus is growing in the frame. The 2 maximum essential sorts of Mucormycosis in this scenario are rhino-orbital-cerebral and pulmonary. [3] The remedy of mucormycosis includes the early initiation of remedy, the surgical debridement of inflamed tissue, antifungal remedy, and coping with the underlying disease.[4] The early signs and symptoms of Rhino-Orbito-Cerebral Mucormycosis are similar to sinusitis and periorbital cellulitis and may document eye and/or facial ache and numbness accompanied via blurred vision.[8] The clinical functions and chest pictures of pulmonary mucormycosis are not particular and difficult to differentiate from pulmonary aspergillosis.[6]
A. Treatment
Amphotericin B (AmB) is the first-line drug of desire; sooner or later, posaconazole and isavuconazole are prescribed.[3] Posaconazole and isavuconazole were used as salvage remedy inside the treatment of mucormycosis.[4] Mucormycosis is a critical infection and desires to be dealt with prescription antifungal medicinal drug, generally amphotericin B, posaconazole, or isavuconazole.
[1] those drug treatments are given thru a vein (amphotericin B, posaconazole, isavuconazole) or with the aid of mouth (posaconazole, isavuconazole).[1] other drug treatments, along with fluconazole, voriconazole, and echinocandins, do no longer paintings in opposition to fungi that reason mucormycosis. Often, mucormycosis calls for surgical procedure to cut away the inflamed tissue.[10] A take a look at from South India assessed the protection and efficacy of posaconazole in ROCM patients. The look at said no mortality; sixty-six.6% of patients had whole decision of the ailment, and the relaxation a great discount of the disease [4]
B. Surgery
Competitive surgical debridement of involved tissues must be taken into consideration as soon because the analysis of any form of mucormycosis is suspected.[13] Surgical intervention with the removal of necrotic tissue and debulking contamination has been related to improved survival in anecdotal clinical evaluations of rhino cerebral and pulmonary contamination.[12] inside the case of rhino cerebral contamination, debridement to put off all necrotic tissue can often be disfiguring, requiring elimination of the palate, nasal cartilage, and the orbit.[13] but, more latest revel in suggests that endoscopic debridement with constrained tissue removal may be completed.[13] There are reviews of patients with early pulmonary infection who had been cured with lobectomies. [12] however, many patients gift with full-size involvement now not amenable to complete resection and/or profound thrombocytopenia, which precludes surgery.[13] In these instances, every attempt need to be made to reverse immunosuppression, optimize underlying scientific conditions, and promptly administer antifungals.[12]
C. Salvage Therapy
We use posaconazole or isavuconazole as salvage remedy for patients who do now not respond to or cannot tolerate amphotericin B. [13] The IV formulation of posaconazole or isavuconazole need to be used in patients who've to be switched from amphotericin B earlier than they have had a favourable reaction and in patients who've an inability to take in oral medicines.[13]
Posaconazole (both IV and behind schedule-release formulations) is given as a loading dose of three hundred mg every 12 hours on the first day, followed through a protection dose of 300 mg every 24 hours thereafter.[13] The IV formula ought to be averted in patients with moderate or excessive renal impairment (creatinine clearance <50 mL/minute) due to the potential for accumulation of the betadex sulfobutyl ether sodium (SBECD) automobile, except an assessment of the viable benefits and risks to the affected person justifies its use.[13] If it's far used in patients with renal impairment, serum creatinine should be monitored intently, and, if will increase occur, attention ought to be given to converting to the extended-launch pill components of posaconazole or to IV or oral isavuconazole.[13] In patients who're capable of taking medications orally, we use posaconazole delayed-release drugs, normally given with meals, in place of the oral suspension because bioavailability with the pills is a great deal better and it's miles less difficult for patients to take.[14]
Isavuconazole has to receive as a loading dose of 200 mg (equivalent to 372 mg of the prodrug isavuconazonium sulfate) IV or orally every 8 hours for the primary six doses accompanied by two hundred mg IV or orally every 24 hours thereafter. Because the IV formula of isavuconazole is especially water soluble and does no longer incorporate the SBECD car, there aren't any recognized concerns about administering the IV method to patients with renal impairment.[14]
The medical efficacy of the oral suspension of posaconazole become shown in a salvage take a look at that enrolled ninety-one patients who had failed or couldn't tolerate trendy therapy.[13] Posaconazole led to a complete or partial response in 60 percent of patients; 21 percent had the solid disease. Even though there are limitations to this salvage have a look at, this collection helps a potential position for oral posaconazole for the treatment of mucormycosis refractory to traditional remedy.[14]
Posaconazole has been described as a second-line remedy in mucormycosis.[17][18] numerous retrospective studies with this antifungal drug have pronounced precise effects. Broadly speaking, this triazole turned into used in patients with failure or intolerance to AmB. The benefits of the oral formula are that it permits in advanced patient discharge and decreases relapse with prolonged management.[19][20] In a prospective study of 21 patients refractory or intolerant to AmB, an excellent reaction turned into stated with posaconazole, apart from patients with disseminated sickness.[21] Posaconazole is usually recommended as second-line treatment for patients with refractory ailment or intolerance to AmB or for folks that want extended treatment protection. The cautioned dose is 400mg bid, and in most said instances therapy is provided for several months [22]
D. Mortality Rate
Mucormycosis is regularly an existence-threatening contamination. An evaluation of published mucormycosis cases observed a universal all-cause mortality fee of 54%.[23]
The mortality fee varied relying on the underlying patient situation, a form of fungus, and the frame web page affected (for example, the mortality charge changed into forty-six% amongst humans with sinus infections, seventy-six% for pulmonary infections, and ninety-six% for disseminated mucormycosis).[23]
Conclusion
Mucormycosis is a developing bellicose fungal disease that requires a high level of clinical skill for a prompt clinical diagnosis in order to improve survival. Where available, new molecular tests should be used to expedite diagnosis. First-line therapy is amphotericin B combined with surgery; second-generation azole derivatives can also be used. Controlling underlying conditions is also an important aspect of therapy.
References
[1] https://www.cdc.gov/fungal/diseases/mucormycosis/index.html#:~:text=Mucormycosis%20(previously%20called%20zygomycosis)%20is,to%20fight%20germs%20and%20sickness. [2] https://www.sciencedirect.com/science/article/pii/S1871402121001570#:~:text=Mucormycosis%20is%20an%20uncommon%20but,Class%2D%20Zygomycetes%20%5B5%5D. [3] https://www.sciencedirect.com/science/article/pii/S1319562X21005775 [4] https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8000977/ [5] https://pubmed.ncbi.nlm.nih.gov/32000287/ [6] Richardson M. The ecology of the Zygomycetes and its impact on environmental exposure external icon. 2009 Oct;15 Suppl 5:2-9. [7] Petrikkos G, Skiada A, Lortholary O, Roilides E, Walsh TJ, Kontoyiannis DP. Epidemiology and clinical manifestations of mucormycosisexternal icon. Clin Infect Dis. 2012 Feb;54 Suppl 1:S23-34. [8] Ribes JA, Vanover-Sams CL, Baker DJ. Zygomycetes in human diseaseexternal icon. Clin Microbiol Rev 2000; 13:236-301. [9] Lewis RE, Kontoyiannis DP. Epidemiology and treatment of mucormycosisexternal icon. Future Microbiol. 2013 Sep;8(9):1163-75. [10] Talmi, YP, Goldschmied-Reouven, A, Bakon, M, Barshack, I, Wolf, M, Horowitz, Z, et al. Rhino-orbital and rhino-orbito-cerebral mucormycosisexternal icon [11] https://en.wikipedia.org/wiki/Mucormycosis#Prevention [12] https://pubmed.ncbi.nlm.nih.gov/23389725/ [13] https://www.cdc.gov/fungal/diseases/mucormycosis/treatment.html#:~:text=How%20is%20mucormycosis%20treated%3F,mouth%20(posaconazole%2C%20isavuconazole). [14] Chander J (2018). \"26. Mucormycosis\". Textbook of Medical Mycology (4th ed.). New Delhi: Jaypee Brothers Medical Publishers Ltd. pp. 534–596 [15] Yamin HS, Alastal AY, Bakri I (January 2017). \"Pulmonary Mucormycosis Over 130 Years: A Case Report and Literature Review\". Turkish Thoracic Journal. 18 [16] Baker RD (March 1957). \"Mucormycosis; a new disease?\". Journal of the American Medical Association. 163 (10): 805–8. [17] Tarani L, Costantino F, Notheis G, Wintergerst U, Venditti M, Di Biasi C, et al. Long-term posaconazole treatment and follow-up of rhino-orbital-cerebral mucormycosis in a diabetic girl. Pediatr Diabetes. 2009;10:289–293. [18] Peel T, Daffy J, Thursky K, Stanley P, Buising K. Posaconazole as first line treatment for disseminated zygomycosis. Mycoses. 2008;51:542–545 [19] Cornely OA, Vehreschild JJ, Rüping MJ. Current experience in treating invasive zygomycosis with posaconazole Treatment Options for Zygomycosis. Clin Microbiol Infect. 2009;15:77–81 [20] Abboud CS, Bergamasco MD, Baía CE, Lallée MP, Zan AS, Zamorano MM, et al. Case Report of Hepatic Mucormycosis After Liver Transplantation : Successful Treatment With Liposomal Amphotericin B Followed by Posaconazole Sequential Therapy. Transplant Proc. 2012;44:2501–2502. [21] Greenberg RN, Mullane K, van Burik JA, Raad I, Abzug MJ, Anstead G, et al. Posaconazole as Salvage Therapy for Zygomycosis. Antimicrob Agents Chemother. 2006;50:126–133. [22] van Burik JA, Hare RS, Solomon HF, Corrado ML, Kontoyiannis DP. Posaconazole Is Effective as Salvage Therapy in Zygomycosis : A Retrospective Summary of 91 Cases. Clin Infect Dis. 2006;42:e61–e65 [23] Roden MM, Zaoutis TE, Buchanan WL, Knudsen TA, Sarkisova TA, Schaufele RL, et al. Epidemiology and outcome of zygomycosis: a review of 929 reported casesexternal icon. Clin Infect Dis. 2005 Sep 1;41(5):634-53.
Copyright
Copyright © 2023 Dhiraj Mundhe, Dr. Rupali Tasgaonkar, Prof. Gayatri Sapkale, Sanskruti Lokhande, Kasturi Turde, Manali Dhule. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.

Download Paper
Paper Id : IJRASET48986
Publish Date : 2023-02-03
ISSN : 2321-9653
Publisher Name : IJRASET
DOI Link : Click Here
 Submit Paper Online
Submit Paper Online