

Ijraset Journal For Research in Applied Science and Engineering Technology
A Study to Assess the Knowledge and Attitude Regarding Preconception Care Among Women in Selected Area of the City With a View to Develop an Information Booklet
Authors: Ms. Archana A Mirzapure, Marylin Shinde
DOI Link: https://doi.org/10.22214/ijraset.2022.46089
Certificate: View Certificate
Abstract
Health is a essential theme in most of the cultures. In fact all communities have their concepts of health, as a part of the individual. The health of the community depends comprehensive health of the all age groups in the community the women, children and old age people health is the indicator whole community health. Health and family welfare services covering the wide spectrum health of all the population. Among this heart of community health depends mainly women’s health. The women’s health depends upon the women in the reproductive age group. Maintaining optimal health is a goal for all women. A quantitative descriptive research approach, survey research design was used in this study to assess the knowledge and attitude regarding preconception care among women in selected area of the city with a view to develop an information booklet. In this study sample consists of 124 women between age group of 18-45 years of age. Structured knowledge questionnaire and attitude scale was developed and introduced to them.
Introduction
I. INTRODUCTION
Essential components of health maintenance are identification of unrecognized problems and potential risks and the education and the health promotion needed to reduce them. This is especially important for women in their childbearing years, because conditions that increase a woman’s health risks are not only of concern for her well-being but also are potentially associated with negative outcomes for both mother and baby in the event of a pregnancy. Prenatal care is an example of prevention that is practiced after conception; however, prevention and health maintenance are needed before pregnancy because many of the mother’s risks can be identified and then eliminated or at least modified.
A. Need For The Study
Major component of Health & Family Welfare Program is related to Health problems of women and children, as they are more vulnerable to ill health and diseases. Since women folk constitute more than 48 % of population, it is essential to health status of women so that the causes of ill health are identified, discussed and misconceptions removed. Ill health of women is mainly due to poor nutrition due to gender discrimination, low age at marriage, risk factors during pregnancy, unsafe, unplanned and multiple deliveries, limited access to family planning methods and unsafe abortion services.10 According to statistics, every minute in the world, 380 women become pregnant 190 face unplanned or unwanted pregnancy; 110 experience a pregnancy-related complication; 40 have an unsafe abortion; and one woman dies from a pregnancy-related cause. Hardly 20per cent of mothers receive all the required components of prenatal care.11 India with its one billion people contributes to about 6.2% of all maternal deaths in the world. To understand the Maternal Mortality situation in the country better and to map the changes, especially at the regional level, the government has categorised states into three groups: empowered action group (EAG), southern states, and other states.12 Even though infant 5 mortality has declined in India maternal mortality has remained high at about 113 per 100,000 live births.
Causes of maternal mortality globally are severe bleeding 25%, Indirect causes 20%, Infection 15%, Unsafe abortions 13%, eclampsia 12%, Obstructed labor 8% and Other direct causes 8%.1 The Indian scenario the maternal mortality is high proportion comparatively other developed countries. The major causes mainly 38% are due to haemarrhage11% sepsis 5% hypertension 5% obstructed labor.1 According to Sample Registration Survey (SRS) in 2016-18, The maternal mortality rate in India is 113 and for Maharashtra is 46 maternal deaths per 1,00,000 women and state has fulfilled the sustainable development goal in this regard set by the United Nations.13
The census of India reported that adolescent girls in the age-group 15-19 years who account for 52.14 million (10.5%) are very sensitive from the viewpoint of planning because of the preparatory stage for their future productive and reproductive roles in the society and family, respectively women in the reproductive age-group 15-44 years numbering 233.72 million (47.1%) need special care and attention because of their reproductive needs.14 In India, more than a million women suffer from RTIs accounting for 25% of the reproductive tract infections between the ages of 15 and 44 years. The main reasons are exist a “culture of silence” surrounding these diseases, due to the associated stigma and taboos as well as the widespread belief that symptoms of pain and discomfort are a natural part of a women’s lifecycle and pre conception health practices.
B. Problem Statement
A study to assess the knowledge and attitude regarding preconception care among women in selected area of the city with a view to develop an information booklet.
C. Objectives of Study
- To assess the knowledge regarding pre conception care among women in selected area of the city.
- To assess the attitude regarding pre conception care among women in selected area of the city.
- To find out the co-relation between knowledge and attitude regarding preconception care among women in selected area of the city.
- To find out the association between knowledge regarding preconception care with selected demographic variables among women in selected area of the city.
- To find out the association between attitude regarding preconception care with selected demographic variables among women in selected area of the city.
D. Assumptions
- There may be inadequate knowledge about preconception care of the woman.
- There may be inadequate attitude towards preconception care of the woman.
E. Ethical Aspect
- The study proposal was sanctioned by ethical committee.
- Confidentiality and anonymity of the sample was obtained.
- Written consent was taken from the participants.
- Prior permission was obtained from the DHO of Urban Health Center.
The nature of the study, aims and objectives were explained to the samples after assuring that their information would be kept confidential and used for research purpose only through written consent of them.
II. RESEARCH METHODOLOGY
- Research Approach: Quantitative descriptive research approach.
- Research Design: descriptive survey research design.
- Setting of the Study: The selected area of the city.
- Target Population: The women of the city.
- Accessible Population: Reproductive age women (18-45 years of age) in selected area of the city.
- Samples: Women (18-45 years) and who fulfilled the inclusion and exclusion criteria.
- Sampling Technique: Non-probability purposive sampling technique.
- Sample Size: 124 women of reproductive age group (18-45 years).
III. CRITERIA FOR SELECTION OF SAMPLE
A. Inclusion Criteria
- Women those who are planning for pregnancy.
- Women who are efficient to read and write English / Marathi.
- The women age group between 18-45 years of age.
B. Exclusion Criteria
- Those who are not willing to participate.
- Those who are not present at the time of study.
- Those who are pregnant.
IV. DESCRIPTION OF TOOL:
A. Section- A
Demographic data of the women Demographic data consist of 10 different variables such as age in years, education, type of family, monthly income of family, occupation, number of children, history of previous pregnancy, information about preconception care, source of information regarding preconception care.
B. Section- B
Structured knowledge questionnaire This tool was prepared by the investigator based on the first objective of the study, that is, to assess the knowledge about preconception care among women. Before preparing the tool, a blueprint was constructed which included 5 different areas such as introduction, general health & fertility, pre-existing medical conditions & drugs, environmental factors, genetic counselling. This tool consists of 30 questions. Scoring mode for structured knowledge questionnaire: Each correct response was given a score of one & incorrect response a score of zero. The maximum scoring possible was 30 & minimum 0 in the knowledge questionnaire.
The scoring was categorized as
0 – 10 = Inadequate knowledge.
11 – 20 = moderate knowledge.
21 – 30 = Adequate knowledge.
C. Section- C
Attitude scale This tool was prepared by the investigator based on the second objective of the study, that is, to assess the attitude towards preconception care among women. It includes 30 items (positive statement-15 and negative statement-15). For positive statements: The responds strongly agree, agree, neutral, disagree, strongly disagree carries 4,3,2,1,0 mark respectively. For negative statements: The responds strongly agree, agree, neutral, disagree, strongly disagree carries 0,1, 2,3,4 marks respectively. The total score was 120120 & minimum 0 in the attitude scale.
The scoring was categorized as:
0-40 = Inadequate attitude
41-80 = Moderate attitude
81-120 = Adequate attitude
V. ORGANIZATION OF STUDY FINDINGS:
- Section I: Frequency distribution of socio demographic variables among women.
- Section II: Assessment of knowledge among women regarding pre conception care.
- Section III: Assessment of attitude among women regarding pre conception care.
- Section IV: Correlate the knowledge and attitude regarding pre conception care among women. Section V: Determine the association between level of knowledge on preconception care with selected demographic variables.
- Section VI: Determine the association between level of attitude on preconception care with selected demographic variables.
Section I: Frequency distribution of socio demographic variables of women.
|
Sr. No |
Demographic Variable |
Category |
Frequency |
% |
|
1 |
Age in Years |
18-22 years |
10 |
8.06 |
|
23-27 years |
81 |
65.32 |
||
|
28-32 years |
29 |
23.39 |
||
|
33-36 Years |
4 |
3.23 |
||
|
36 & above |
0 |
0.00
|
||
|
2 |
Education |
Illiterate |
4 |
3.23 |
|
Primary |
5 |
4.03 |
||
|
Secondary |
11 |
8.87 |
||
|
Higher secondary |
23 |
18.55 |
||
|
Graduation |
74 |
59.68 |
||
|
PG & above |
7 |
5.65 |
||
|
3 |
Type of Family |
Joint |
57 |
45.97 |
|
Nuclear |
67 |
54.03 |
||
|
4 |
Diet Pattern |
Vegetarian |
80 |
64.52 |
|
Mixed |
44 |
35.48 |
||
|
5 |
Income |
Below Rs 15000/- |
1 |
0.81 |
|
Rs. 15001-Rs. 25000 |
5 |
4.03 |
||
|
Rs. 25001-Rs 35000 |
51 |
41.13 |
||
|
Above Rs 35000 |
67 |
54.03 |
||
|
6 |
Occupation |
Housewife |
41 |
33.06 |
|
Government |
42 |
33.87 |
||
|
|
|
|
||
|
Private Job |
41 |
33.06 |
||
|
Business |
0 |
0.00 |
||
|
7 |
Number of Children |
No any |
6 |
4.84 |
|
1 |
96 |
77.42 |
||
|
2 |
21 |
16.94 |
||
|
>2 |
1 |
0.81 |
||
|
8 |
History of previous pregnancy |
Abortion |
3 |
2.42 |
|
Congenital anomaly |
1 |
0.81 |
||
|
Still birth |
1 |
0.81 |
||
|
LBW |
5 |
4.03 |
||
|
Normal outcome |
111 |
89.52 |
||
|
Any other |
3 |
2.42 |
||
|
9 |
Do you know about preconception care |
Yes |
113 |
91.13 |
|
No |
11 |
8.87 |
||
|
10 |
If Yes, Source of information |
Social Media |
18 |
15.93 |
|
Health care professional |
55 |
48.67 |
||
|
Friends & family |
40 |
35.40 |
||
|
any other |
0 |
0.00 |
The above table 1 interprets, out of 124 samples, majority of the samples 81(65.32%) belongs to 23-27 years age group, 29(23.39%) belongs to 28-32 years age group, 10(8.06%) belongs to 18-22 years age group 4(3.23%) belongs to 33-36 years and none of the sample were age group of 36 years and above.
With regards to education, majority of the samples 74(59.68%) were graduates, 23(18.55%) were studied higher secondary education, 11(8.87%) were secondary education, 7(5.65%) were post graduates and above, 5(4.03%) were primary education and 4(3.23%) were illiterate.
Regarding type of family, majority of the sample 67(54.03%) were nuclear family type and 57(45.97%) were residing joint family.
With regards to diet pattern, majority of the samples 80(64.52%) were vegetarian and 44(35.48%) were mixed diet pattern.
Regarding Income of the family, 67(54.03%) were earning above Rs. 35000/-, 51(41.13%0 were earning Rs. 25001- Rs 35000/-, 5(4.03%) were having monthly income of Rs. 15001- Rs 25000/- and 1(0.81%) was earning below Rs. 15000/-.
With regards to occupation of the women, 42(33.87%) were in government employee, 41(33.06%) each in private and house wives and none of the samples were business as a occupation.
Regarding number of children, 96(77.42%) were having 1 child, 21(16.94%) were having 2 children, 6(4.84%) were not having child and 1(0.81%) was having above 2 children.
With regards to history of previous pregnancy, majority of the sample 111(89.52%) were having a normal outcome history, 5(4.03%) were low birth weight pregnancy history, 3(2.42%) each in abortion and any other history and 1(0.81%) each in congenital anomaly and still birth as a history of pregnancy.
With regards to information regarding preconception care among women, majority of the women 113(91.13%) were having information regarding it whereas 11(8.87%) were does not have any information about preconception care.
Regarding source of information in concern to preconception care, majority of the sample 55(48.67%) were heard with health care professional, 40(35.40%) heard through friends and family, and 18(15.93%) by social media.
Section II: Assessment of knowledge among women regarding pre conception care
|
Level of knowledge regarding preconception care |
Score |
Frequency |
Percentage (%) |
Mean |
SD |
|
Inadequate knowledge |
0-10 |
5 |
4.03 |
18.90 |
3.40 |
|
Moderate knowledge |
11-20 |
69 |
55.64 |
||
|
Adequate knowledge |
21-30 |
50 |
40.32 |
Table no 2 shows that, majority of the samples 69(55.64%) were having moderate level of knowledge, 50(40.32%) were having adequate knowledge and 5(4.03%) had inadequate knowledge on pre conception care.
Section III: Assessment of attitude among women regarding pre conception care
|
Level of attitude regarding preconception care |
Score |
Frequency |
Percentage (%) |
Mean |
SD |
|
Inadequate Attitude |
0-40 |
13 |
10.48 |
58.88 |
9.95 |
|
Moderate Attitude |
41-80 |
104 |
83.87 |
||
|
Adequate Attitude |
81-120 |
7 |
5.64 |
Table no 3 shows that, majority of the samples 104 (83.87%) were having moderate attitude, 7 (5.64%) were having adequate attitude and 13(10.48%) had inadequate attitude towards pre conception care.
Section IV: Correlate the knowledge and attitude regarding pre conception care among women
|
DOMAIN |
CORRELATION BETWEEN |
MEAN SCORE |
KARL PEARSON CORRELATION COEFFICIENT (r) |
P |
|
Mean ± SD |
||||
|
Preconception Care among Women |
Knowledge versus attitude score |
18.90 ± 3.40 Versus 58.88 ± 9.95 |
0.54 |
0.000* |
Table no 4 shows, knowledge and attitude scores with correlation value 0.54, there was a positive correlation with a significant level of 0.05.
A. Frequency distribution of level of knowledge and attitude
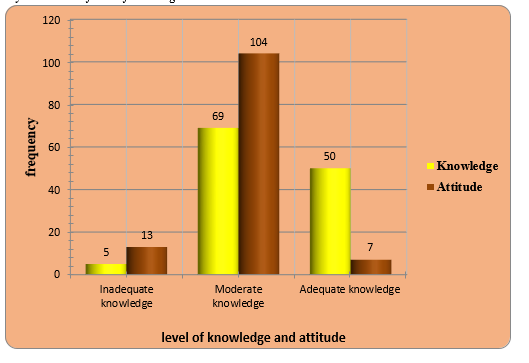
B. Figure Showing Frequency Distribution Of Level Of Knowledge And Attitude Score Among Women
Figure shows that, majority of the sample 104(83.87%) were having moderate attitude, whereas 69(55.64%) were having moderate knowledge, 50(40.32%) were having adequate knowledge where as 7(5.64%) were having adequate attitude and 13(10.48%) were having inadequate attitude whereas 5(40.3%) were having inadequate knowledge.
C. Association Between Level Of Attitude With Selected Demographic Variables
n=124
|
Sr. NO |
Demographic Variables |
Attitude on Preconception care |
df |
Chi square Value |
P Value |
Significance |
||
|
Inadequate Attitude |
Moderate Attitude |
Adequate Attitude |
||||||
|
1 |
Age in Years |
|||||||
|
18-22 years |
3 |
7 |
0 |
6 |
7.53 |
0.274 |
Not Significance |
|
|
23-27 years |
7 |
71 |
4 |
|||||
|
28-32 years |
2 |
23 |
3 |
|||||
|
33-36 Years |
1 |
3 |
0 |
|||||
|
36 & above |
0 |
0 |
0 |
|||||
|
2 |
Education |
|||||||
|
Illiterate |
4 |
0 |
0 |
10 |
150.522 |
0.0000 |
Significance |
|
|
Primary |
5 |
0 |
0 |
|||||
|
Secondary |
3 |
8 |
0 |
|||||
|
Higher secondary |
1 |
22 |
0 |
|||||
|
Graduation |
0 |
72 |
2 |
|||||
|
PG & above |
0 |
2 |
5 |
|||||
|
3 |
Type of Family |
|||||||
|
Joint |
13 |
43 |
1 |
2 |
19.004 |
0.00 |
Significance |
|
|
Nuclear |
0 |
61 |
6 |
|||||
|
4 |
Type of Diet |
|||||||
|
Vegetarian |
12 |
63 |
5 |
2 |
5.237 |
0.052 |
Not Significance |
|
|
Mixed |
1 |
41 |
2 |
|||||
|
5 |
Income |
|||||||
|
Below Rs 15000/- |
0 |
1 |
0 |
6 |
11.405 |
0.076 |
Not Significance |
|
|
Rs. 15001-Rs. 25000 |
1 |
4 |
0 |
|||||
|
Rs. 25001-Rs 35000 |
10 |
40 |
1 |
|||||
|
Above Rs 35000 |
2 |
59 |
6 |
|||||
|
6 |
Occupation |
|||||||
|
Housewife |
11 |
30 |
0 |
4 |
22.2007 |
0.000 |
Significance |
|
|
Government |
0 |
37 |
5 |
|||||
|
Private Job |
2 |
37 |
2 |
|||||
|
Business |
0 |
0 |
0 |
|||||
|
7 |
No Children |
|||||||
|
No any |
0 |
6 |
0 |
6 |
6.894 |
0.330 |
Not Significance |
|
|
1 |
9 |
83 |
4 |
|||||
|
2 |
4 |
14 |
3 |
|||||
|
>2 |
0 |
1 |
0 |
|||||
|
8 |
History of previous pregnancy |
|||||||
|
Abortion |
0 |
3 |
0 |
10 |
1.945 |
0.996 |
Not Significance |
|
|
Congenital anomaly |
0 |
1 |
0 |
|||||
|
Still birth |
0 |
1 |
0 |
|||||
|
LBW |
1 |
4 |
0 |
|||||
|
Normal outcome |
12 |
94 |
7 |
|||||
|
Any other |
0 |
1 |
0 |
|||||
|
9 |
Do you have information regarding preconception care |
|||||||
|
Yes |
10 |
96 |
7 |
2 |
4.105 |
0.128 |
Not Significance |
|
|
No |
3 |
8 |
0 |
|||||
|
10 |
If Yes, Source of information |
|||||||
|
Social Media |
1 |
15 |
2 |
4 |
1.746 |
0.782 |
Not Significance |
|
|
Health care professional |
5 |
48 |
2 |
|||||
|
Friends & family |
4 |
33 |
3 |
|||||
|
any other |
0 |
0 |
0 |
|||||
The table 6 describes that, association between level of attitude score on pre conception care among women with selected demographic variables. The study demographic variables were; education, type of family, and occupation were significant, where as age, type of diet, income, number of children, history of previous pregnancy, information regarding pre conception care and source of information were not significant.
In order to compute the association between the level of knowledge score and demographic variables chi-square was applied and the value was observed with 0.05 significance level.
The chi square value of education χ =150.52 with 10 degree of freedom, type of family χ=19.00 with 2 degree of freedom, type of diet χ= 5.23 with 2 degree of freedom and occupation χ=22.20 with 4 degree of freedom found statistically significant with demographic variable. Whereas there was no other demographic variables found association with level of attitude score on preconception care.
VI. DISCUSSION
The knowledge and attitude was assessed by structured knowledge questionnaire and attitude scale. Knowledge and attitude scores with correlation value 0.54, there was a positive correlation with a significant level of 0.05. A similar cross-sectional study was carried out by Pritesh G Patel, Tejas A Shah At Urban Areas of Vadodara City, Gujarat, India among 100 newly married women residing at urban area of Vadodara city, To assess the knowledge & attitude regarding preconceptional care of newly married women of selected urban area of Vadodara city. The women were interviewed by using structured questionnaire. Data analysis was done using Microsoft Excel.
Out of 100 interviewed women 12% had poor, 82% had average and 6% of women had good knowledge. 52% of women had negative attitude and 48% of women had positive attitude. Correlation between knowledge and attitude was 0.815 at 5% level of significance which suggest moderately positive correlation. Average knowledge, Negative attitude & moderately positive correlation regarding pre-conceptional care were noticed among newly married women.
Conclusion
The knowledge and attitude was assessed by structured knowledge questionnaire and attitude scale. The conclusion drawn from the findings of the study are as follows: Majority of the samples were having moderate level of knowledge. Majority of the samples were having moderate level of attitude. There was a positive correlation between knowledge and attitude scores with correlation value 0.54, with a significant level of 0.05. The association between level of knowledge with selected demographic variables was significant in Education, type of family, income, occupation, and source of information regarding preconception care. The association between level of attitude with selected demographic variables was significant in Education, type of family, and occupation.
References
[1] K. Park. Preventive and Social medicine. 19th edition, Banardass Bhanot publishers.page no. [2] Report from Institute for Research in Reproduction (IRR), Mumbai, the network of Human Reproduction Research Centres (HRRCs) 2003-2004.www.google.com [3] K.K. Gulani. Community Health Nursing Principles and Practices. Kumar Publishing House first edition 2005; pp no 339-350 [4] http://www.bbc.co.uk/parenting/having_a_baby/ [5] http://www.marchofdimes.com/professionals/14332_1156.asp#top july 2008 [6] Lowdermilk, Perry, Cashion, Alden, Maternity & Women’s Health, 10th edition, Elsevier Mosby. Page no:70 [7] Meeting to develop a global consensus on Preconception care to reduce maternal and childhood mortality and morbidity Geneva, World Health Organization, 2013 [8] Cuco G, Arija V, Iranzo R et al. Association of maternal protein intake before conception and throughout pregnancy with birth weight. Acta Obstet Gynecol Scand. 2006;85(4):413-21 [9] Han A, Rotermann M, Fuller-Thomson E.et.at. Preconceptional folic acid supplement use according to maternal country of birth. Journal of Obstetric Gynecology of Cannada. 2009 March;31(3):222-6 [10] Ministry Health and family welfare of India annual report 2006-2007 [11] Asha Krishna Kumar. public health- unsafe motherhood. Volume 21 - issue 16, July. 31 - August13, 2004.india\'s national magazine. from the publishers of the Hindu. [12] The Hindu: maternal death rate declining report,8th November 2019 [13] The New Indian Express, Maharashtra retains second spot in maternal mortality rate, 16 July 2020. [14] Census of India, 2001: Provisional Population Totals, Registrar-General & Census Commissioner, Government of India, New Delhi [15] Greene, M. E., M. Mehta, J. Pulerwitz, D. Wulf, A. Bankole, and S. Singh (2006) “Involving Men in Reproductive Health: Contributions to Development.” Paper prepared for the UN Millennium Project to contribute to the report Public Choices, Private Decisions: Sexual and Reproductive Health and the Millennium Development Goals [16] de Jong-Potjer LC, de Bock GH, et al.Women\'s interest in GP-initiated preconception counseling in The Netherlands. Family Practioner. 2003 April;20(2):142-6. [17] Pande, R., Kurz K.,Jain et al. Improving Reproductive Health of Married and Unmarried Youth in India. ICRW Publication: 2006. Washington, DC, USA. [18] Abdella FG, Levine E. Better patient care through nursing research, 3rd edition; Newyork; Macmillan publishing:1986 [19] Pender’s Health Promotion Model- Nursing theory; complementary counterpart to models of health promotion;1995 [20] B.T. Basavantappa. Text book of research.5th edition. New Delhi: Jaypee brothers medical publishers; 2008.
Copyright
Copyright © 2022 Ms. Archana A Mirzapure, Marylin Shinde . This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.

Download Paper
Paper Id : IJRASET46089
Publish Date : 2022-07-30
ISSN : 2321-9653
Publisher Name : IJRASET
DOI Link : Click Here
 Submit Paper Online
Submit Paper Online