

Ijraset Journal For Research in Applied Science and Engineering Technology
Case Study: Snakebite Envenomation in Toddler and Acute Abdomen
Authors: Ms. Blessy Mathew, Ms. Sanju Solanki
DOI Link: https://doi.org/10.22214/ijraset.2022.47582
Certificate: View Certificate
Abstract
The Child aged 10 year was bought to the Emergency Department of Chhatrapati Subharti Hospital with the chief complaints of no body movement which was diagnosed as the case of cardiac arrest as per the evidences suggested by recordings of vital parameters. History taken from the father revealed the toddler boy had a snake bite in middle finger of the left hand. After wards child complained of severe abdominal pain and the entire body got collapsed and they rushed to hospital as a lifesaving attempt, where CPR was initiated in hospital first which was followed by the emergency treatment in the form of administration of Anti snake venom Anti serum and after wards the child was admitted in paediatric ICU and was on the medical treatment for 10 days and on after which the boy was shifted to general ward and 15th day he got discharged.
Introduction
I. INTRODUCTION
Snake bite is one of the neglected public health issue in many tropical and subtropical countries. About 5.4 million snake bites occur each year, resulting in 1.8 to 2.7 million cases of envenoming (poisoning from snake bites). There are between 81 410 and 137 880 deaths and around three times as many amputations and other permanent disabilities each year. Bites by venomous snakes can cause acute medical emergencies involving severe paralysis that may prevent breathing, cause bleeding disorders that can lead to fatal haemorrhage, cause irreversible kidney failure and severe local tissue destruction that can cause permanent disability and limb amputation. Children may suffer more severe effects, and can experience the effects more quickly than adults due to their smaller body mass.
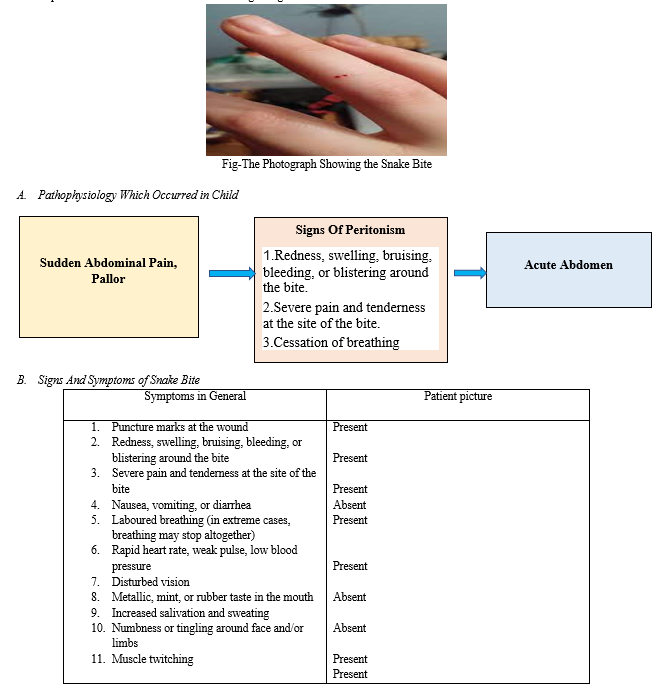
II. UNDERLYING GENERAL PATHOPHYSIOLOGY
Snake venoms 90% of dry weight comprises greater than 100 different proteins: enzymes, non-enzymatic polypeptide toxins, and non-toxic proteins. Enzymes mainly are digestive hydrolases, hyaluronidase (spreading factor), yellow L-amino acid oxidases, phospholipases A2 , and peptidases. Snake venom metalloproteases (SVMPs) damage basement membranes, causing endothelial cell damage and spontaneous systemic bleeding. Procoagulant enzymes which are present are thrombin-like, splitting fibrinogen, or activators of factors V, X, prothrombin and other clotting factors, causing DIC, consumption coagulopathy and incoagulable blood. Phospholipases A2 which is also present damage mitochondria, red blood cells, leucocytes, platelets, peripheral nerve endings, skeletal muscle, vascular endothelium, and other membranes, producing presynaptic neurotoxic activity, cardiotoxicity, myotoxicity, necrosis, hypotension, haemolysis, anti-coagulation, haemorrhage, plasma leakage (oedema formation) and auto pharmacological release of histamine and other autacoids. Also, Polypeptide postsynaptic (α) neurotoxins bind to acetylcholine receptors at the motor endplate and Presynaptic (β) neurotoxins are phospholipases that damage nerve endings irreparably.
III. CASE DESCRIPTION
The child aged 10 year was bought to the emergency department of Chhatrapati Subharti Hospital with the chief complaints of no body movement which was diagnosed as the case of cardiac arrest as per the evidences suggested by recordings of vital parameters. After which Immediately the CPR was conducted and intubation was been done. Meanwhile the history taking from parents of the child revealed that the child had snake bite in left hand middle finger and afterwards he complained of severe abdominal pain and afterwards he collapsed by going into cardiac arrest. In emergency ward after initiation of CPR with the administration of Emergency Drugs including Adrenaline immediately Anti Snake Venom Anti serum was given to the child. And when after wards the vital parameters got stable the child was shifted to paediatric ICU where the rest of the treatment where given.
The treatment was continued and after 6 hours there was mild eyebrow movement was been made, which was followed by thumb and lastly foot movement but entire body tonicity was absent.
After 6 days the child was extubated with oxygen and oral sips were allowed and medications were also been given and after wards on the 10 day he got shifted to paediatric ward where rest of the treatment continued and after 5 days he got discharged from the hospital. As there was neither peritonitis nor intraperitoneal free fluid. There was no mesenteric lymph node. Other abdominal organs were essentially normal. No surgical act was performed. The child was only given the intravenous medications including broad spectrum antibiotics and medications for regaining the muscle tone.
C. Management Carried Out
- Day 1 – Day 5
a. Child, NPO was treated on the ventilator SIMU mode with adrenaline support
b. Antibiotics -Inj Vancomycin, and Inj. Ceftriaxone were given in paediatric doses
c. Antacids -including Inj Pantop
d. Neuromuscular Stimulators -Inj Atropin, Neostigmine
e. Antipyretics- Inj.PCM
f. IV fluids to maintain hydration
2. Day 6-Day10
a. Extubate the child with oxygen.
b. Antibiotics -Inj Vancomycin, and Inj. Meropenam ,Inj colistin were given in Paediatric doses
c. Antacids -Including Inj Pantop
d. Antiemetics- Inj.Emset
e. Antipyretics- Inj.PCM
f. IV fluids to maintain hydration
3. Day 10-Day 15
a. The child was allowed orally
b. Antibiotics -Inj Ceftriaxone in paediatric doses
c. Intake output charting was maintained
IV. PROGNOSIS
As the vital parameter got stable and the cardiac arrest has been revived. And anti-snake venom Anti serum has been given in time. also, Since There was neither peritonitis nor intraperitoneal free fluid and There was no mesenteric lymph node which was observed. Other abdominal organs were essentially normal so no surgery was performed. Although the Initially child was kept in Paediatric ICU after 10 days the condition of the toddler started improving and on the 15 day the toddler got discharged.
Conclusion
Pain abdomen is one of the most commonly encountered complaints in paediatric emergency room. The child had a sudden onset abdominal pain, and later went on to develop neuro-muscular paralysis and respiratory failure. The root cause was found to be snake-bite. The child had a stormy course but full recovery was made after getting full and through medical Intervention.
References
[1] KangC, Kim DH, Kim SC, Kim DS, Jeong CY. Atraumatic splenic rupture after coagulopathy owing to a snake bite. Wilderness and Env Med 2014: 25, 325-8 [2] Tchaou BA, Tové KS De, Tové YS De, Djomga ATC, Aguemon A, Massougbodji A, et al. Contribution of ultrasonography to the diagnosis of internal bleeding in snake bite envenomation. J Venom Anim Toxins Incl Trop Dis 2016;22:1-7. [3] Belonwu RO, Gwarzo GD. Envenomation secondary to facial snake bite:Report of a rare occurrence. Niger J Paediatr. 2015;42 :162-4. [4] Kim JS, Yang JW, Kim MS, Han ST, Kim BR, Shin MS, et al. Coagulopathy in patients who experience snakebite. Korean J Intern Med 2008;23:94-9. [5] Njoku CH, Isezuo SA, Makusidi MA. An audit of snake bite injuries seen at the Usmanu Danfodiyo University Teaching Hospital, Sokoto, Nigeria. Nig Pg Med J 2008;15:112-5. [6] Marsh N, Williams V. Practical application of snake venom toxins in haemostasis. Toxicon 2005;45:1171-81 [7] Marsh N, Williams V. Practical application of snake venom toxins in haemostasis. Toxicon 2005;45:1171-81 [8] Kularatne SA. Common krait (Bungarus caeruleus) bite in Anuradhapura, Sri Lanka: a prospective clinical study, 1996-98. Postgrad Med J 2002; 78:276-80 [9] Dixon RW, Harris JB. Nerve terminal damage by beta-bungarotoxin: its clinical significance. Am J Pathol 1999; 154: 447-455. [10] Kularatne SA. Common krait (Bungarus caeruleus) bite in Anuradhapura, Sri Lanka: a prospective clinical study, 1996-98. Postgrad Med J 2002; 78:276-280
Copyright
Copyright © 2022 Ms. Blessy Mathew, Ms. Sanju Solanki. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.

Download Paper
Paper Id : IJRASET47582
Publish Date : 2022-11-21
ISSN : 2321-9653
Publisher Name : IJRASET
DOI Link : Click Here
 Submit Paper Online
Submit Paper Online